
Association between temperature and volume of emergency medical service response due to injury in Chengdu
-
摘要:背景
伤害是重要的公共卫生问题之一,在气候变化的背景下研究气温与伤害的关联,对伤害防控具有重要意义。
目的探讨成都市气温与伤害120急救量的关联。
方法采用回顾性生态学方法,从成都市气象局收集2022年1月1日—2023年12月31日成都市气象数据,包括日均气温、日均相对湿度、平均风速、平均气压、日照及降雨量,从成都市120急救中心获取同期全市120急救数据,应用分布滞后非线性模型分析气温与伤害120急救量的关联,并根据不同性别、年龄进行分层分析,探索不同人群对气温的敏感性。
结果共收集到2022—2023年成都市伤害120急救人数为
219685 人,伤害原因前三位依次为交通事故、中毒和跌坠伤,急救量分别为90765 (41.32%)、44101 (20.07%)、44046 (20.05%)。日均气温在17.9 ℃以上时,随着温度增高,伤害120急救量也升高。在单日滞后效应中,日均气温与伤害120急救量的关联开始于滞后第一天(lag1),一直持续到lag6,其效应最大值出现在lag2、lag3和lag4;以17.9 ℃为参照,日均气温每升高1 ℃,伤害120急救量均增加1.08倍,95%CI 分别为1.03~1.14、1.04~1.12和1.04~1.16。男性和女性均易受气温的影响,但在相同滞后日,男性的RR值均高于女性。日均气温对0~17岁年龄组在整个滞后期内的效应均无统计学意义;对18~44岁年龄组的效应出现在lag1~lag6;对45~64岁年龄组的效应出现在lag1~lag4;65岁及以上年龄组的效应仅体现在lag3(RR : 1.05,95%CI : 1.00~1.10)。结论成都市气温升高时伤害120急救量也有所增加,尤其在男性和18~44岁人群中的关联更强。
Abstract:BackgroundInjury is a major public health issue, and studying the correlation between temperature and injury in the context of climate change is of great significance for injury prevention and control.
ObjectiveTo analyze the association between temperature and the volume of emergency medical service response due to injury in Chengdu.
MethodsUsing a retrospective ecological study design, weather data in Chengdu were collected from 1 January 2022 to 31 December 2023 from Chengdu Meteorological Office, including daily average temperature, daily average relative humidity, average wind speed, average pressure, sunshine, and rainfall. Emergency medical service data were collected from an emergency medical service center in Chengdu. A distributional lag non-linear model was conducted to calculate the association between temperature and volume of emergency medical service response due to injury, and gender- and age-stratified analyses were followed to identify susceptible groups.
ResultsOverall
219685 incidents of emergency medical service dispatching due to injury were collected during the study period. The top three injury causes were traffic accident (90765 , 41.32%), poisoning (44101 , 20.07%), and falling (44046 , 20.05%). When daily average temperature exceeded 17.9 ℃, as the temperature rised, the volume of emergency medical service response for injury increased. In terms of the single-day lag effect, the risk of emergency medical service response for injury elevated on lag1 and persisted until lag6, the maximum daily effectwas observed on lag2, lag3 and lag4, and their relative risks associated with every 1℃ higher above 17.9 ℃ were both 1.08 times, 95%CIs were (1.03, 1.14), (1.04, 1.12), and (1.04, 1.16) respectively. Both men and women were susceptible to temperature, but on the same lag day, the men's RR value was higher than the women's. There was no statistical difference in the lag effect of temperature on the 0-17 age group; the lag effect on the 18-44 age group appeared on lag1, and lasted to lag6; that for the 45-64 age group appeared on lag1, and lasted to lag4; that for the 65 age group and over was only on lag 3 (RR: 1.05, 95%CI: 1.00, 1.10).ConclusionAs the temperature rises, the volume of emergency medical service response due to injury is increased in Chengdu. In particular, the associated impact is significant on males and people aged 18-44 years old.
-
伤害是一个不可忽视的公共卫生问题,据世界卫生组织估计,全球每年约有440万人死于伤害[1]。在我国,伤害是第五大死亡原因[1]。根据目前全世界通用的国际疾病分类(International Classification of Diseases, ICD)第10次修订本(ICD-10)以及伤害的相关研究[2–3],伤害包括:交通事故、中毒、跌坠伤、器械伤、溺水、烧烫伤、蛰咬伤、电击伤、意外机械性窒息等。伤害作为人群前五位死因之一,不仅对人群的健康产生严重影响,对社会卫生资源也造成了大量的损耗[4–5]。
随着全球气候变化,环境温度呈现上升的趋势,有研究表明,非适宜气温会对人体的呼吸系统、心血管系统等产生不良影响,从而增加人群发病风险[6–7],甚至导致死亡人数增加[8–9]。环境温度在对人体内在健康产生影响的同时,也与人群的伤害发生率相关[1]。有研究显示,环境温度的变化会增加道路交通事故的风险[10]。伤害属于环境温度对人群健康的短期效应之一[11–12],研究气温与伤害的关联具有重要现实意义。
成都市地处四川盆地,受亚热带季风气候的影响,具有春短、夏热、秋凉、冬暖等气候特点。本研究基于成都市气象资料和伤害急救资料,分析气温与伤害120急救量的关联,旨在为公众在气温变化情况下预防伤害的发生提供相应的应对措施,为本地区开展预防伤害的公共卫生干预提供科学依据。
1. 材料与方法
1.1 资料来源
本研究所用的气象数据来源于成都市气象局,包括日均气温、日均相对湿度、平均风速、平均气压、日照及降雨量。急救数据来源于成都市120急救中心,涵盖成都市所有区县,包括:接诊日期、患者性别、年龄、住址、呼救地址、接诊时主诉、初步诊断等。本研究已取得四川省疾病预防控制中心伦理委员会审查批准(编号:SCCDCIRB第2024-005号)。
1.2 数据筛选
从成都市120急救中心获取2022年1月1日至2023年12月31日全市急救数据,结合接诊时主诉和初步临床诊断,同时参考ICD-10标准中损伤、中毒和外因的某些其他后果(S00-T98)以及疾病和损伤的外因(V01-Y99),筛选出包含伤害相关字段的患者。排除标准:病例资料不完整影响结果判断的病例;疾病所致伤害病例,如肿瘤、心脑血管疾病等。
1.3 数据质量控制
气象数据来源于成都市气象局,2022年1月1日至2023年12月31日共包含730个自然日,缺失了3个自然日的数据,使用前后两日均值进行填补。由于收集的伤害急救数据没有包括ICD编码,故采用双人根据关键字段进行筛选的方法,使筛选出的数据中每日病例数保持一致。
1.4 统计分析
1.4.1 描述性分析
本研究属于回顾性生态学研究。使用EXCEL 2022 软件进行数据填补和筛选,采用SPSS 23.0统计软件对伤害120急救量的人口统计学特征和气象数据进行描述汇总。
1.4.2 时间序列分析
气温与伤害120急救量的关联分析使用R 4.3.1软件,采用相对危险度RR(95%CI)表示气温与伤害120急救量的关联,分析均采用双侧检验,检验水准α设定为0.05。采用时间序列分析方法,基于分布滞后非线性模型(distributed lag non-linear models, DLNM)进行分析。模型公式为:
$$ \begin{split} &\mathrm{Log[E(} \mathit{Y} _{ \mathit{t} } \mathrm{]=} {\alpha } \mathrm+ \mathit{cb} {({\rm{Temp}},l)+} \mathit{ns} \mathrm{(WeatherConfounders,} {\nu } \mathrm{)+} \\ &\qquad\mathit{ns} \mathrm{(time,} {\nu } \mathrm{)+DOW+Holiday} \end{split} $$ 式中,Yt代表第t天伤害120急救人数;α为截距;cb(Temp, l )为气温和滞后天数的交叉基,其中l为最长滞后天数;ns为自然立方样条函数;WeatherConfounders为纳入模型控制的气象因素(相对湿度、气压、日照、风速、降雨量),ν为自由度,通常取值为3[13];time为时间序列数据的顺序,用以调整长期趋势和季节性,自由度ν为7/年[14];DOW为星期几效应;Holiday为节假日效应。气象因素对机体健康的影响滞后时间较短,一般滞后时长为1~7 d[11](后文表示为lag1~lag7),因此本研究选择最长滞后天数为7 d。根据赤池信息准则(Quasi-Akaike Information Criterion, quasi-AIC)选择最优模型,确定交叉基函数中的自由度。以日均气温的中位数作为参考温度用于效应分析[15]。
1.4.3 敏感性分析
为验证模型的稳定性,通过改变模型中样条函数的时间自由度和相对湿度的自由度进行敏感性分析。
2. 结果
2.1 一般情况
2022—2023年成都市日均气温的均数±标准差($\bar x \pm s $)为(17.5±1.4)℃。期间共收集伤害120急救人数
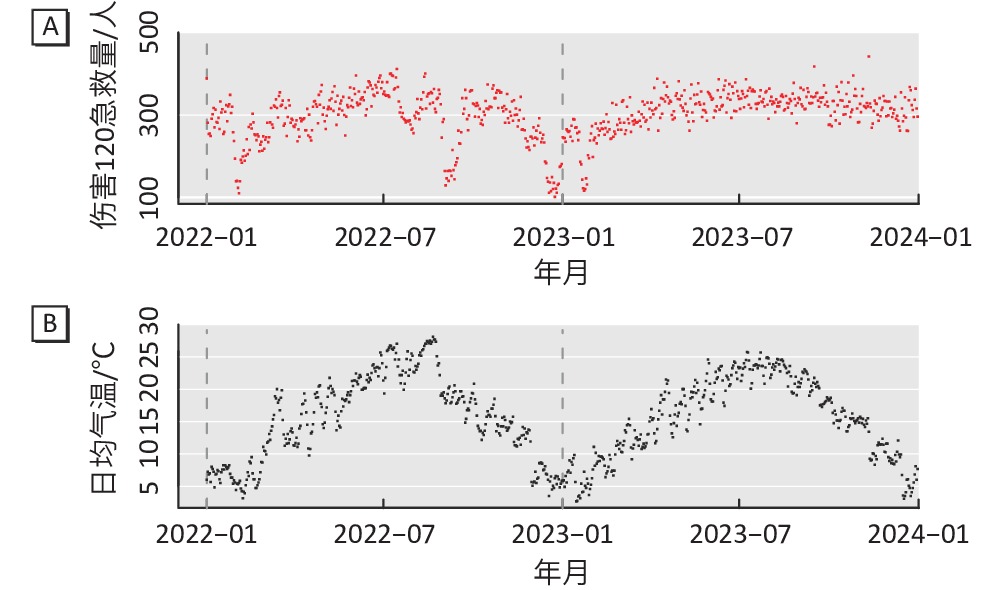
219685 人,其中男性134266人 (61.12%),女性85419人 (38.88%);日均急救人数为(300.9±65.8)人(表1)。伤害原因前三位依次为交通事故、中毒和跌坠伤,急救量分别为90765 (41.32%)、44101 (20.07%)、44046 (20.05%)。从气象因素和伤害120急救量的时序图来看,夏季日均气温升高,伤害相关的120急救量也增多,二者变化趋势基本一致(图1)。表 1 2022—2023年成都市伤害120急救情况及气象因素Table 1. Volume of emergency medical service response due to injury and meteorological factors in Chengdu from 2022 to 2023变量 $\bar x \pm s $ 最小值 最大值 P25 P50 P75 伤害120急救量/(人·d−1) 总人群 300.9±65.8 101 442 274.5 314.0 339.0 性别 男性 183.9±50.9 52 284 167.3 190.0 209.0 女性 117.0±14.8 38 185 104.0 120.0 132.0 年龄/岁 0~17 18.3±9.2 1 39 14.0 18.0 23.0 18~44 146.2±98.3 24 223 129.0 152.5 171.0 45~64 84.9±50.2 19 144 76.0 86.0 96.0 ≥65 50.7±20.5 20 88 44.0 50.0 57.0 气象因素(n=730) 日均气温/℃ 17.5±1.4 2.2 32.7 11.1 17.9 23.9 日均相对湿度/% 77.2±4.1 34.2 97.5 71.1 78.0 84.2 平均气压/hpa 949.1±4.8 933.9 971.3 942.7 949.3 955.2 风速/(m·s−1) 1.4±0.1 0.6 4.0 1.1 1.3 1.6 日照/(h·d−1) 3.3±4.2 0.0 12.5 0.0 1.6 6.3 降雨量/(mm) 2.7±0.8 0.0 100.4 0.0 0.0 1.0 ![]() 图 1 2022—2023年成都市伤害120急救量(A)与日均气温(B)的时序分布图Figure 1. The time-series distribution of emergency medical service response volume (A) and daily mean temperature (B) in Chengdu from 2022 to 2023
图 1 2022—2023年成都市伤害120急救量(A)与日均气温(B)的时序分布图Figure 1. The time-series distribution of emergency medical service response volume (A) and daily mean temperature (B) in Chengdu from 2022 to 20232.2 日均气温与伤害120急救量的暴露-反应关系
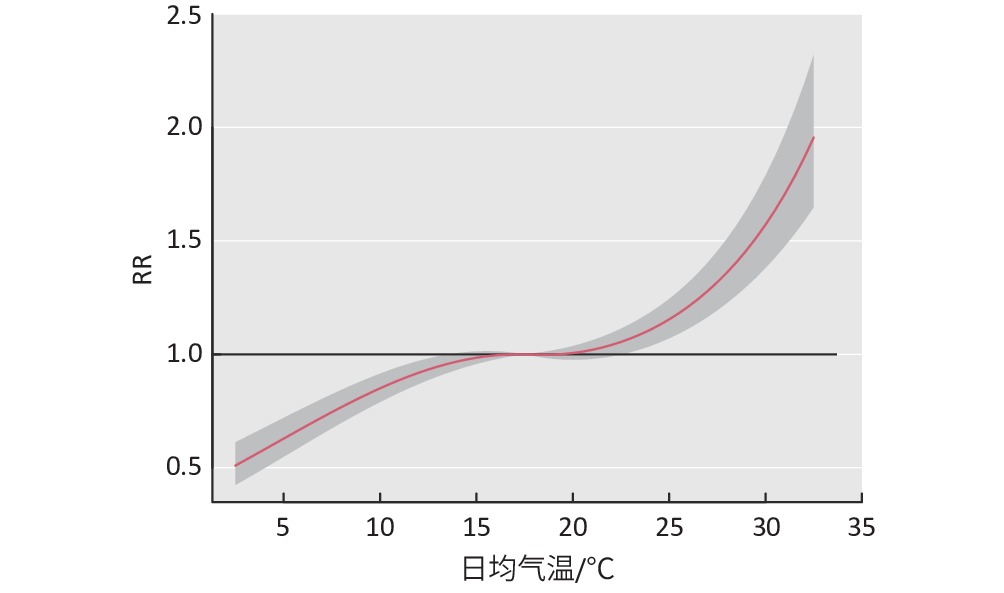
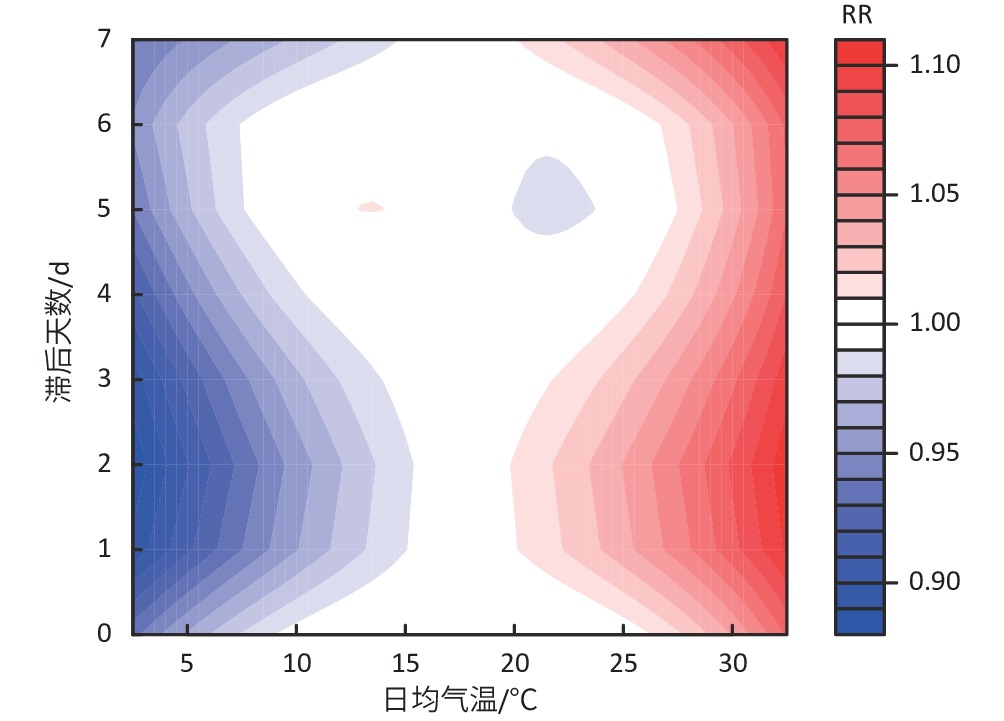
如图2所示,以日均气温的中位数(17.9 ℃)作为参考温度,在17.9 ℃以上时,日均气温与伤害120急救量的暴露-反应关系呈近似线性递增,即随着温度增高,伤害120急救量也增高。如图3所示,在单日滞后效应中,日均气温对伤害120急救的效应开始于lag1,一直持续到lag6,其效应最大值出现在lag2、lag3和lag4;以17.9 ℃为参照,日均气温每升高1 ℃,伤害120急救量均增加1.08倍,95%CI分别为1.03~1.14、1.04~1.12和1.04~1.16(表2)。
![]() 图 2 2022—2023年成都市日均气温与伤害120急救量的暴露-反应关系图Figure 2. Exposure-response relationship between the number of emergency medical service response and daily mean temperature in Chengdu from 2022 to 2023
图 2 2022—2023年成都市日均气温与伤害120急救量的暴露-反应关系图Figure 2. Exposure-response relationship between the number of emergency medical service response and daily mean temperature in Chengdu from 2022 to 2023![]() 图 3 不同滞后天数的气温与伤害120急救量RR值关系的等高线图Figure 3. Contour map of the exposure-lag-response relationship between the number of emergency medical service response and daily mean temperature表 2 2022—2023年成都市气温对伤害120急救量的相对危险度[RR(95%CI)]Table 2. Relative risk of the number of emergency medical service response in association with daily mean temperature in Chengdu from 2022 to 2023 [RR(95%CI)]
图 3 不同滞后天数的气温与伤害120急救量RR值关系的等高线图Figure 3. Contour map of the exposure-lag-response relationship between the number of emergency medical service response and daily mean temperature表 2 2022—2023年成都市气温对伤害120急救量的相对危险度[RR(95%CI)]Table 2. Relative risk of the number of emergency medical service response in association with daily mean temperature in Chengdu from 2022 to 2023 [RR(95%CI)]组别 lag0 lag1 lag2 lag3 lag4 lag5 lag6 Lag7 总人群 1.06 (0.98 ~1.16) 1.07 (1.03~1.12)* 1.08 (1.03~1.14)* 1.08 (1.04~1.12)* 1.08 (1.04~1.16)* 1.07 (1.02~1.12)* 1.05 (1.01~1.09)* 1.03 (0.95~1.12) 性别 男性 1.05 (0.96~1.16) 1.08 (1.04~1.13)* 1.10 (1.04~1.16)* 1.10 (1.05~1.14)* 1.09 (1.05~1.13)* 1.07 (1.02~1.14)* 1.06 (1.01~1.11)* 1.05 (0.95~1.15) 女性 1.08 (0.98~1.19) 1.06 (1.02~1.11)* 1.06 (1.00~1.12)* 1.06 (1.02~1.10)* 1.06 (1.02~1.10)* 1.06 (1.00~1.12)* 1.04 (1.00~1.09)* 1.02 (0.93~1.12) 年龄/岁 0~17 1.12 (0.89~1.40) 1.05 (0.95~1.16) 1.03 (0.90~1.17) 1.03 (0.94~1.12) 1.04 (0.95~1.14) 1.06 (0.94~1.21) 1.09 (0.98~1.20) 1.10 (0.88~1.36) 18~44 1.09 (0.97~1.22) 1.09 (1.03~1.15)* 1.09 (1.02~1.17)* 1.09 (1.04~1.14)* 1.09 (1.04~1.14)* 1.09 (1.01~1.16)* 1.08 (1.02~1.13)* 1.06 (0.95~1.19) 45~64 1.05 (0.93~ 1.19) 1.08 (1.02~1.14)* 1.08 (1.01~1.16)* 1.08 (1.02~1.13)* 1.06 (1.01~1.11)* 1.05 (0.98~1.12) 1.04 (0.98~1.10) 1.04 (0.93~1.17) ≥65 0.98 (0.88~1.10) 1.03 ( 0.98~1.09) 1.05 (0.99~1.12) 1.05 (1.00~1.10)* 1.04 (0.99~1.09) 1.02 (0.96~1.09) 1.01 (0.96~1.07) 1.02 (0.91~1.14) [注] 参照温度(17.9 ℃);*:P<0.05。 2.3 不同特征分层分析
亚组分析结果显示,男性和女性均易受气温的影响,但在相同滞后日,男性的RR值均高于女性。日均气温对0~17岁年龄组在整个滞后期内的效应值均无统计学意义;对18~44岁年龄组的效应与总人群基本一致,体现在lag1~lag6;对45~64岁年龄组的效应体现在lag1~lag4;65岁及以上年龄组的效应仅体现在lag3(RR:1.05,95%CI:1.00~1.10)(表2)。
2.4 敏感性分析
lag2和lag3为全人群有统计学意义的最强效应滞后时间,从亚组效应滞后时间来看,lag3为18~44岁、45~64岁以及65岁及以上3个年龄组均有效应的时间,因此选择lag3改变模型中时间样条函数的自由度(5~7)和相对湿度的自由度(2~4)进行敏感性分析,气温对伤害120急救量的影响变化不大,说明该模型稳定性较好。见表3。
表 3 2022—2023年成都市气温与伤害120急救量关系的敏感性分析(RR,95%CI)Table 3. Sensitivity analysis between the number of emergency medical service response and daily mean temperature in Chengdu from 2022 to 2023变量 滞后日 自由度 RR 95%CI 时间 lag3 5 1.08 1.04~1.11 6 1.08 1.04~1.12 7 1.08 1.04~1.12 相对湿度 lag3 2 1.08 1.04~1.12 3 1.08 1.04~1.12 4 1.08 1.05~1.12 3. 讨论
本研究采用分布滞后非线性模型分析了2022—2023年成都市气温与伤害120急救量的关联,结果显示,以日均气温的中位数(17.9 ℃)作为参考温度,在17.9 ℃以上时,日均气温与伤害120急救量的暴露-反应关系呈近似线性递增,即随着温度增高,伤害120急救量也增高,效应最大值出现在lag2、lag3和lag4,与深圳市[16]的研究中高温是伤害120急救量的危险因素结论一致。但在健康效应研究方面,气温对人群疾病的效应主要呈“U”型或“V”型[17–18],这与本研究有所不同,差异的原因主要在于疾病的病因不同于伤害,从低温到最适温度,人群患病风险逐渐降低[7],而在伤害的相关研究中,占比最大的是交通事故[1,19],在本研究中,交通事故导致的伤害占41.32%。适宜气候条件下,人群的出行反而增多,交通量增加,出行方式也增加,比如步行和骑行等,这些因素都有可能导致伤害风险增加。有实验研究表明,在炎热的天气下机体的5-羟色胺分泌受到抑制[20],可能引起决策能力下降,增加伤害事件的发生,如交通事故、职业伤害或跌倒等[1]。高温或室内外温差过大还会使个体情绪波动幅度增大,从而诱发暴力伤害等行为[21]。
流行病学研究证实,对气候变化的易感性因性别和年龄而异[22]。本研究中,男性和女性均易受气温的影响,但在相同滞后日,男性的RR值均高于女性,而且从伤害120急救人数来看,男性多于女性,比例约为1.6:1,与大多数城市的研究结果是一致的[23–24]。伤害病因前3位依次为:交通事故、中毒和跌坠伤。在交通驾驶员群体中,大多为男性;中毒的类型大部分为急性酒精中毒,而男性群体更喜喝酒;再加上社会分工不同,男性更多从事户外工作,比如运输、快递、外卖等接触高温天气概率更大的职业,发生交通事故和摔伤的风险也更高。综合以上原因,在相同气温和滞后天数的情况下,男性发生伤害120急救的风险值要高于女性。
有研究表明,年龄是伤害的独立危险因素,同时还与生理因素及心理行为因素相互影响[25]。在本研究中,从效应持续时间来看,日均气温对0~17岁年龄组在整个滞后期内的效应均无统计学意义,18~44岁年龄组的滞后效应与总人群基本一致,45~64岁年龄组的效应持续时间短于18~44岁年龄组;65岁以上年龄组的效应仅体现在第3天。这与以往的研究中中青年是伤害发生的主要群体结论相似。0~17岁年龄组包括学龄前儿童和中小学生,这两类群体基本以室内活动为主,外出频率较低,因此发生伤害急救的风险也相对较低。成都市作为一个相对“年轻化”的都市,18~44岁年龄组和45~64岁年龄组是社会的主要劳动力,有一定比例从事运输、快递、外卖等城市保障工作的青壮年人群以及从事建筑、绿化、环卫等工作的中老年人群,相较于老年人,这些人群暴露于高温环境的频率更高,是伤害发生的高危群体[26]。
本研究的不足之处:首先,气象数据来源于成都市气象局的监测站点,离监测站点较远的人群,其暴露的环境温度可能跟监测站点的温度有一定差异。其次,伤害的发生受到气候、个体生理特征以及生活行为方式等多方面的影响[27],本研究属于生态学研究的范畴,来源于急救中心的伤害数据,接诊记录中没有病人的病史、生活方式等信息,在分析过程中无法对这些因素进行调整控制。最后,本研究收集的伤害病例仅来源于120急救中心,可能存在部分发生伤害的病例未前往医院就诊,导致收集到的伤害病例低于实际伤害病例,气温的健康效应被低估。
综上所述,2022—2023年成都市气温增高会增加伤害120急救风险,尤其在夏季高温期间,有必要提醒公众采取预防伤害的有效措施。
-
![]()
图 1 2022—2023年成都市伤害120急救量(A)与日均气温(B)的时序分布图
Figure 1. The time-series distribution of emergency medical service response volume (A) and daily mean temperature (B) in Chengdu from 2022 to 2023
![]()
图 2 2022—2023年成都市日均气温与伤害120急救量的暴露-反应关系图
Figure 2. Exposure-response relationship between the number of emergency medical service response and daily mean temperature in Chengdu from 2022 to 2023
![]()
图 3 不同滞后天数的气温与伤害120急救量RR值关系的等高线图
Figure 3. Contour map of the exposure-lag-response relationship between the number of emergency medical service response and daily mean temperature
表 1 2022—2023年成都市伤害120急救情况及气象因素
Table 1 Volume of emergency medical service response due to injury and meteorological factors in Chengdu from 2022 to 2023
变量 $\bar x \pm s $ 最小值 最大值 P25 P50 P75 伤害120急救量/(人·d−1) 总人群 300.9±65.8 101 442 274.5 314.0 339.0 性别 男性 183.9±50.9 52 284 167.3 190.0 209.0 女性 117.0±14.8 38 185 104.0 120.0 132.0 年龄/岁 0~17 18.3±9.2 1 39 14.0 18.0 23.0 18~44 146.2±98.3 24 223 129.0 152.5 171.0 45~64 84.9±50.2 19 144 76.0 86.0 96.0 ≥65 50.7±20.5 20 88 44.0 50.0 57.0 气象因素(n=730) 日均气温/℃ 17.5±1.4 2.2 32.7 11.1 17.9 23.9 日均相对湿度/% 77.2±4.1 34.2 97.5 71.1 78.0 84.2 平均气压/hpa 949.1±4.8 933.9 971.3 942.7 949.3 955.2 风速/(m·s−1) 1.4±0.1 0.6 4.0 1.1 1.3 1.6 日照/(h·d−1) 3.3±4.2 0.0 12.5 0.0 1.6 6.3 降雨量/(mm) 2.7±0.8 0.0 100.4 0.0 0.0 1.0  下载: 导出CSV
下载: 导出CSV
表 2 2022—2023年成都市气温对伤害120急救量的相对危险度[RR(95%CI)]
Table 2 Relative risk of the number of emergency medical service response in association with daily mean temperature in Chengdu from 2022 to 2023 [RR(95%CI)]
组别 lag0 lag1 lag2 lag3 lag4 lag5 lag6 Lag7 总人群 1.06 (0.98 ~1.16) 1.07 (1.03~1.12)* 1.08 (1.03~1.14)* 1.08 (1.04~1.12)* 1.08 (1.04~1.16)* 1.07 (1.02~1.12)* 1.05 (1.01~1.09)* 1.03 (0.95~1.12) 性别 男性 1.05 (0.96~1.16) 1.08 (1.04~1.13)* 1.10 (1.04~1.16)* 1.10 (1.05~1.14)* 1.09 (1.05~1.13)* 1.07 (1.02~1.14)* 1.06 (1.01~1.11)* 1.05 (0.95~1.15) 女性 1.08 (0.98~1.19) 1.06 (1.02~1.11)* 1.06 (1.00~1.12)* 1.06 (1.02~1.10)* 1.06 (1.02~1.10)* 1.06 (1.00~1.12)* 1.04 (1.00~1.09)* 1.02 (0.93~1.12) 年龄/岁 0~17 1.12 (0.89~1.40) 1.05 (0.95~1.16) 1.03 (0.90~1.17) 1.03 (0.94~1.12) 1.04 (0.95~1.14) 1.06 (0.94~1.21) 1.09 (0.98~1.20) 1.10 (0.88~1.36) 18~44 1.09 (0.97~1.22) 1.09 (1.03~1.15)* 1.09 (1.02~1.17)* 1.09 (1.04~1.14)* 1.09 (1.04~1.14)* 1.09 (1.01~1.16)* 1.08 (1.02~1.13)* 1.06 (0.95~1.19) 45~64 1.05 (0.93~ 1.19) 1.08 (1.02~1.14)* 1.08 (1.01~1.16)* 1.08 (1.02~1.13)* 1.06 (1.01~1.11)* 1.05 (0.98~1.12) 1.04 (0.98~1.10) 1.04 (0.93~1.17) ≥65 0.98 (0.88~1.10) 1.03 ( 0.98~1.09) 1.05 (0.99~1.12) 1.05 (1.00~1.10)* 1.04 (0.99~1.09) 1.02 (0.96~1.09) 1.01 (0.96~1.07) 1.02 (0.91~1.14) [注] 参照温度(17.9 ℃);*:P<0.05。
下载: 导出CSV
表 3 2022—2023年成都市气温与伤害120急救量关系的敏感性分析(RR,95%CI)
Table 3 Sensitivity analysis between the number of emergency medical service response and daily mean temperature in Chengdu from 2022 to 2023
变量 滞后日 自由度 RR 95%CI 时间 lag3 5 1.08 1.04~1.11 6 1.08 1.04~1.12 7 1.08 1.04~1.12 相对湿度 lag3 2 1.08 1.04~1.12 3 1.08 1.04~1.12 4 1.08 1.05~1.12
下载: 导出CSV
-
[1] HU J, HE G, MENG R, et al. Temperature-related mortality in China from specific injury[J]. Nat Commun, 2023, 14(1): 37. doi: 10.1038/s41467-022-35462-4
[2] DE RAMIREZ S S, HYDER A A, HERBERT H K, et al. Unintentional injuries: magnitude, prevention, and control[J]. Annu Rev Public Health, 2012, 33: 175-191. doi: 10.1146/annurev-publhealth-031811-124558
[3] JIN Z, HAN B, HE J, et al. Unintentional injury and its associated factors among left-behind children: a cross-sectional study[J]. BMC Psychiatry, 2023, 23(1): 478. doi: 10.1186/s12888-023-04964-w
[4] LUO L, ZENG F, BAI G, et al. Future injury mortality burden attributable to compound hot extremes will significantly increase in China[J]. Sci Total Environ, 2022, 845: 157019. doi: 10.1016/j.scitotenv.2022.157019
[5] DUAN L, YE P, HAAGSMA J A, et al. The burden of injury in China, 1990-2017: findings from the Global Burden of Disease Study 2017[J]. Lancet Public Health, 2019, 4(9): e449-e461. doi: 10.1016/S2468-2667(19)30125-2
[6] TRAN H M, CHUANG T W, CHUANG H C, et al. Climate change and mortality rates of COPD and asthma: a global analysis from 2000 to 2018[J]. Environ Res, 2023, 233: 116448. doi: 10.1016/j.envres.2023.116448
[7] WEN J, ZOU L, JIANG Z, et al. Association between ambient temperature and risk of stroke morbidity and mortality: a systematic review and meta-analysis[J]. Brain Behav, 2023, 13(7): e3078. doi: 10.1002/brb3.3078
[8] HEALY J P, DANESH Y M, WEI Y, et al. Seasonal temperature variability and mortality in the medicare population[J]. Environ Health Perspect, 2023, 131(7): 77002. doi: 10.1289/EHP11588
[9] YU X, WANG Y, HE C, et al. The trend of unintentional injury-related mortality among children aged under-five years in China, 2010-2020: a retrospective analysis from a national surveillance system[J]. BMC Public Health, 2023, 23(1): 673. doi: 10.1186/s12889-023-15546-6
[10] AHMED S K, MOHAMMED M G, ABDULQADIR S O, et al. Road traffic accidental injuries and deaths: a neglected global health issue[J]. Health Sci Rep, 2023, 6(5): e1240. doi: 10.1002/hsr2.1240
[11] LIANG M, ZHAO D, WU Y, et al. Short-term effects of ambient temperature and road traffic accident injuries in Dalian, Northern China: a distributed lag non-linear analysis[J]. Accid Anal Prev, 2021, 153: 106057. doi: 10.1016/j.aap.2021.106057
[12] ZHENG H, CHENG J, HO H C, et al. Evaluating the short-term effect of ambient temperature on non-fatal outdoor falls and road traffic injuries among children and adolescents in China: a time-stratified case-crossover study[J]. Front Environ Sci Eng, 2023, 17(9): 105. doi: 10.1007/s11783-023-1705-1
[13] HU Y, CHENG J, JIANG F, et al. Season-stratified effects of meteorological factors on childhood asthma in Shanghai, China[J]. Environ Res, 2020, 191: 110115. doi: 10.1016/j.envres.2020.110115
[14] BHASKARAN K, GASPARRINI A, HAJAT S, et al. Time series regression studies in environmental epidemiology[J]. Int J Epidemiol, 2013, 42(4): 1187-1195. doi: 10.1093/ije/dyt092
[15] MENG L, ZHOU C, XU Y, et al. The lagged effect and attributable risk of apparent temperature on hand, foot, and mouth disease in Changsha, China: a distributed lag non-linear model[J]. Environ Sci Pollut Res Int, 2023, 30(5): 11504-11515.
[16] 邝小娜. 深圳市2013~2017年气象因素对意外伤害120急救量的影响[D]. 武汉: 华中科技大学, 2021. KUANG X N. The influence of meteorological factors on the volume of first aid for accidental injury in Shenzhen, 2013~2017[D]. Wuhan: Huazhong University of Science and Technology, 2021.
[17] LUONG L M T, PHUNG D, SLY P D, et al. Effects of temperature on hospitalisation among pre-school children in Hanoi, Vietnam[J]. Environ Sci Pollut Res Int, 2019, 26(3): 2603-2612. doi: 10.1007/s11356-018-3737-9
[18] XIA Y, SHI C, LI Y, et al. Effects of ambient temperature on mortality among elderly residents of Chengdu city in Southwest China, 2016-2020: a distributed-lag non-linear time series analysis[J]. BMC Public Health, 2023, 23(1): 149. doi: 10.1186/s12889-022-14931-x
[19] World Health Organization. Injuries and violence[EB/OL]. [2024-07-20]. https://www.who.int/news-room/fact-sheets/detail/injuries-and-violence.
[20] VORONOVA I P. 5-HT receptors and temperature homeostasis[J]. Biomolecules, 2021, 11(12): 1914. doi: 10.3390/biom11121914
[21] PALINKAS L A, WONG M. Global climate change and mental health[J]. Curr Opin Psychol, 2020, 32: 12-16. doi: 10.1016/j.copsyc.2019.06.023
[22] 宇传华, 吴思齐. 基于全球视角的中国伤害负担现状及趋势分析[J]. 公共卫生与预防医学, 2019, 30(3): 1-6. YU C H, WU S Q. From the global views to analyze status and trend of injury burden in China[J]. J Pub Health Prev Med, 2019, 30(3): 1-6.
[23] YIN Q, WANG J. A better indicator to measure the effects of meteorological factors on cardiovascular mortality: heat index[J]. Environ Sci Pollut Res Int, 2018, 25(23): 22842-22849. doi: 10.1007/s11356-018-2396-1
[24] GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017[J]. Lancet, 2018, 392(10159): 1789-1858. doi: 10.1016/S0140-6736(18)32279-7
[25] XU Z, ETZEL R A, SU H, et al. Impact of ambient temperature on children's health: a systematic review[J]. Environ Res, 2012, 117: 120-131. doi: 10.1016/j.envres.2012.07.002
[26] 陈非儿, 东春阳, 张江华, 等. 2013—2023年热浪对上海居民中暑的影响[J]. 环境与职业医学, 2024, 41(6): 610-616. doi: 10.11836/JEOM23407 CHEN F E, DONG C Y, ZHANG J H, et al. Effects of heat waves on heat stroke in Shanghai, 2013—2023[J]. J Environ Occup Med, 2024, 41(6): 610-616. doi: 10.11836/JEOM23407
[27] SCHWEBEL D C. Why “accidents” are not accidental: using psychological science to understand and prevent unintentional child injuries[J]. Am Psychol, 2019, 74(9): 1137-1147. doi: 10.1037/amp0000487
计量
- 文章访问数: 78
- HTML全文浏览量: 13
- PDF下载量: 22

